News
Summary
Peyronie’s disease is a condition that is usually observed by patients with a bent penis due to a connective tissue disorder and it is more common than you think. The bent penis may cause painful erections and makes it impossible for men to have sex without pain. There are a variety of causes for the said condition which includes trauma, and genetics. One might suspect that they have Peyronie’s but it would be best to consult with a doctor and have an ultrasound to be sure. There are different ways to treat the condition with surgical and non-surgical ways.
saltirewise What is Peyronie’s disease?
Peyronie’s disease is a condition that is often observed by patients with a bent penis. It is a connective tissue disorder that involves the development of fibrous plaques, often due to scar tissue, in the penis.
This scar tissue creates an abnormal bent looking penis.
The curvature of the penis normally during erection is due to the pressure the plaque causes on the surrounding tissues. This curvature or bending may cause painful erections.
Ultimately, this condition may make it impossible or painful for a man to have sex.
It must be emphasized that having a curved erection alone does not imply that this condition is present.
where can i buy Clomiphene from in the uk What are the symptoms of Peyronie’s disease?
The symptoms of Peyronie’s may come and go or develop slowly. The pain usually reduces with time, but the shape and curvature of the penis may not change. Additionally, there is a tendency for men to have erectile dysfunction and other problems during intercourse. One of the common symptoms of this disease are as follows:
- Pain: Men may experience sharp or mild pain in their penis during an erection. In some cases, men may experience this even without an erection. The pain experienced can be traced to inflammation in the fibrotic plaque. Some patients report that this pain may spontaneously resolve within one year.
- Shortening of the penis: Peyronie’s can result in a noticeable decrease in the size of a man’s penis. Due to shrinkage or shortening of the penis, patients may opt to undergo surgery, which is a reasonable step to take once one is diagnosed with this condition.
- Obvious bend in the penis: There may be a change in the shape of the penis. It may either point in the upward or downward direction. This curve or bend is due to the formation of plaques under the skin of the penis.
- Abnormal looking penis: A common symptom may also be any “abnormal” change in the appearance of the penis. Some men experience a thickening of the base of the penis or an hourglass looking penis. The scar tissue can create a large range of abnormalities in the penis.
- Feeling of scar tissue: This tissue is not visible. However, it is palpable under the skin as a bulge of hard tissue or lump. It should be noted that this is one of the most common signs in men.
- Erectile dysfunction: It is described as the incapacity of men to retain an erection so that it stays stiffened for sex. This condition is commonly described among men with the disease and as such all men who come through Vityl men’s health clinic are screened for Peyronie’s disease.
These symptoms may progress or go away. Over time, the condition may improve, however, the pain may take 24 to 36 months to clear up. However, shortening and curvature may not disappear.
How does Peyronie’s Cause ED?
Research shows that it is not definite whether or not men with Peyronie’s disease will have erectile dysfunction, but ED is a common occurrence among males with the disease. The following are some factors that may significantly point to erectile disorders are:
- The weakening of the smooth muscle tissue on the penis due to plaques or plaques may make it difficult for an erection to occur.
- Plaques may affect the flow of blood into the penis, which ultimately leads to a stiff erection.
- Blood may flow out of the penis at a high rate, which ultimately leads to the loss of erection.
As much as 20% to 54% of men with Peyronie’s disease report experiencing erectile dysfunction.
Because of the deformity, you may experience difficulty in maintaining erectile function and inability to sustain intercourse.
However, one must also consider that ED may be a possible adverse effect of Peyronie’s disease surgical treatment. After corrective surgery for Peyronie’s, the new incidence of erectile dysfunction ranges from;
- 4% to 13% for plication procedures and
- 5% to 53% for grafting surgery
How does Peyronie’s effect your quality of life?
Men who suffer from Peyronie’s disease almost instantly begin to experience negative effects on their self-esteem, confidence and enjoyment in the bedroom.
These changes in the appearance and function of the penis can be associated with emotional and psychosocial consequences, leading to an negative impact on your quality of life.
Psychologically, Peyronie’s disease may cause depression in men. This state of depression occurs due to their situation or condition. It ultimately leads them into anxiety and fear before sexual activity. Sometimes, they may be terrified by the thought of sex itself. Depression, anxiety, and fear of sexual activities can result in erectile dysfunction in men.
Men may find this condition very disgraceful and embarrassing; however, patients must be reassured that seeing an expert is a vital step in getting adequate and appropriate treatment. The doctor will help manage the condition and provide the best course of treatment.
Is Peyronie’s painful?
In men, Peyronie’s disease could lead to high levels of pain. Typically, it becomes more common with age. Often, men with this condition may develop sexual issue, which ultimately leads to depression or anxiety.
What causes Peyronie’s disease?
Although the cause of Peyronies disease is still being investigated it has been shown that Peyronie’s disease can be caused by;
- trauma
- inflammation
- hormones
- genetics
- a combination of the above
Trauma to your penis can cause Peyronies disease. The most common inciting event is thought to be microvascular trauma to the penile shaft associated with penile buckling in the erect or semi-erect state secondary to sexual activity. However, many patients do not recall an incident that preceded the onset of symptoms.
One study initially suggested that the disease results from a series of mild inflammatory and fibrosing reactions secondary to urethritis. Urethritis is inflammation of the urethra. That’s the tube that carries urine from the bladder to outside the body. Pain with urination is the main symptom of urethritis. Urethritis is commonly due to infection by bacteria. It is supported by studies which suggest that Peyronie’s disease begins with an acute inflammatory process. If prolonged, the inflammatory response will result in the remodelling of connective tissue into a dense fibrotic plaque.[10]
However, the most recent accepted view is that PD is a form of fibromatosis. Fibromatosis is the name given to a group of soft tissue tumours that change the consistency of the tissue. The causes of fibromatosis remains unclear. In some types of fibromatosis, it is thought that the condition may be related to trauma, hormonal factors, or have a genetic association.
It is hypothesized that fibrosis results from a cascade of biological reactions, which is incited by repetitive minor trauma to the penis.
These changes then lead to transformation in the tunical collagen from type 1 to a predominant type 3. The inciting trauma is also associated with subsequent inelasticity of the tunica leading to scarring.
How common is Peyronie’s disease?
Peyronie’s is more common than you think.
Prevalence of Peyronie’s disease varies widely, however, worldwide prevalence estimates range from 0.3% to 13.1%.
Rates may be higher among men who present with comorbidities such as those with diabetes, prostate cancer, hypertension, lipid abnormalities, ischaemic cardiomyopathy, erectile dysfunction, smoking, and excessive consumption of alcohol.
Studies have shown that the prevalence can be as high as 16% in men after radical prostatectomy and up to 20.3% in men with diabetes and erectile dysfunction.
It is believed that Peyronie’s disease is under-reported due to factors such as a lack of knowledge on the disease, social stigma, as well as inability to recognize that the disease may be occurring on a spectrum of symptoms.
Am I at risk of getting Peyronie’s disease?
Peyronie’s diseases is not always caused by injury or trauma. Some potential causes of Peyronie’s include;
- Age: Your risk of developing Peyronie’s disease increases with age and is quite high for men in their 50’s and 60’s. Some men are born with Peyronie’s or develop it very early. These men are diagnosed as having congenital penile curvature.
- Genes: It is thought that Peyronie’s disease has a hereditary link and if one of your family members has PD then you have a higher chance of developing it.
- Connective tissue disorders: If you already have connective tissue disorders around your hands or elsewhere you are at greater risk of developing Peyronie’s disease.
- Lifestyle: Poor lifestyle choices such as drinking and smoking are thought to increase the chances of developing PD and increase the severity of exiting cases.
How do you diagnose Peyronie’s disease?
Peyronie’s disease is relatively simple to diagnose. At Vityl Men’s Health Clinic we have uncovered undiagnosed Peyronie’s disease through a series of examinations and questions about your medical history. Once an initial diagnosis has been made our doctors may schedule a scan and a referral with our urologist to discuss treatment options.
How can you self-diagnose Peyronie’s disease?
Most times, people may be scared to seek consultation with a doctor once they notice any of the common symptoms. It should be noted that speaking to a doctor is the best way to find out whether or not you have this condition. It must be emphasized that if you do notice any of these symptoms below, you must consider seeking a formal diagnosis sooner rather than later.
The symptoms of Peyronie’s disease include:
- Overnight shortening of the penis
- Lumps in the penis
- Soft erections
- Narrowing or “hourglass” of the penile shaft
- Painful erections during sexual intercourse
- A curve in the penis during an erection.
How do you formally diagnose Peyronie’s?
A patient may notice certain signs and symptoms which may indicate Peyronie’s disease. Some of these symptoms include pain, abnormal shape, lumps in the penis, and shrinking or decrease in length, among many others.
In some cases, the medical experts may need to trace the cause of the noticeable changes before making specific conclusions. During the investigation, some patients may recall incidents which incurred an injury to the penis during sexual intercourse or other vigorous activities.
The standard evaluation of Peyronie’s disease requires a thorough medical history and by the doctor or the patient performing a physical examination. Accurate measurement of penile curvature is vital for monitoring progression of disease, treatment planning, and improvement.
Do I need an ultrasound or xray?
Ultrasound YES.
X-Ray NO.
At times when the symptoms may seem inconclusive, an ultrasound can be helpful. The use of ultrasound is effective and painless and will capture pictures of soft tissues that are not visible enough on X-rays.
The imaging tests function by sending sound waves, magnetic fields, and other forms of energy through the body. They are critical in gathering additional data about the plaque.
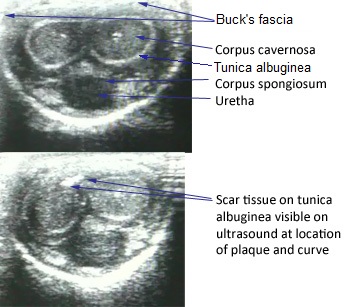
Peyronie’s disease: Unaffected penis V’s affected penis
Does my doctor need to do a physical examination?
Maybe.
What happens during a physical examination is the urologist or GP starts the examination by feeling plaques in the penis either with or without an erection. If there’s a need for a physical examination with an erection, the doctor may inject an agent that causes erections.
It is advisable that all patients take images of their erect penis at home in order to observe, analyze, and monitor changes.
How critical is my family history?
Family history either helps reduce the risk of health problems or increase it. The primary purpose of this step is to identify members of the family that have similar conditions. Experts believe that Peyronie’s disease may have a significant effect on an individual with similar family occurrences. Hence, men with a family history of Peyronie’s may develop the disease, however, this data is still under investigation. The medical experts may ask of the following questions:
- When did you start seeing signs of a curve or scar tissue?
- Do you feel pain with or without an erection?
- Do you have problems keeping an erection or issues having sex?
- Are there people in your family that have this condition or any other similar medical condition?
- Are you on any specific treatment? If you are, may you list them?
- Do you have underlying medical conditions or problems?
Peyronie’s disease treatment
While diagnosing Peyronie’s disease is easy. Treatment can be quite complicated and may include surgery.
Will Peyronie’s go away on it own?
It is rare for Peyronie’s disease to heal by itself. Normally, the condition either remains the same or gets worse. This is why we suggest you contact an expert as soon as you experience symptoms of Peyronie’s or ED. Studies show that when it gets treated early, there is a lower probability of it worsening. Moreover, immediate treatment can improve very serious symptoms like penile shortening, curvature, and pain.
In 2014, a study by Berookhim and his colleagues showed that among 176 men with uniplanar penile curvature who opted for no treatment, sixty-seven percent did not experience a change in the curvature upon follow-up after 12 months. Meanwhile, only 12% experienced an improvement, and 21% reported worsened penile curvature.
Those who did not experience any change were more likely to be older men who have had symptoms for greater than six months, while those who reported improvement were younger individuals who have had symptoms for less than six months.
Additional data also suggest that for many or most patients, penile pain will resolve over time even without intervention; and that curvature and other types of deformity are less likely to improve and may require treatment.
When should I get Peyronie’s treated?
It is important to get treatment for Peyronie’s as soon as possible.
Clinically, it is useful to distinguish between patients who have active disease and those who have stable disease because the type of treatment would depend on whether the patient’s symptoms are dynamic or stable.
- Active Peyronie’s Disease is characterized by changing symptoms, such as penile pain or discomfort with or without erection, which is the determining symptom of the active stage. The onset of this stage may occur alongside a history of penile buckling during intercourse. Additionally, the patient may or may not experience penile induration, which is a palpable plaque associated with painful penile deformity and possible curvature.
- On the other hand, stable Peyronie Disease is characterized by symptoms which have been unchanged for at least three months based on either patient report or clinician documentation. The patient may experience penile pain with or without an erection, but is less common than that experienced by those with active disease. In addition, in this stage of the disease, the deformity is no longer progressive.
Non-surgical treatment methods
A recommended treatment procedure is dependent on the period during which an individual experiences the symptoms. The acute phase of this condition doesn’t require any form of surgery. It is characterized by penile pain that lasts between two, three weeks, and sometimes twelve months or more. Effective non-surgical treatments include:
- Penile traction therapy: This therapy stops potential shrinking and reduces the degree of curvature
- Medical and injection therapies: In some cases, this may work better for certain people and might be ineffective for others.
The penile traction therapy deals with the use of a self-applied device to stretch the penis. It helps improve curvature and penile length. For the best results, these devices need to remain intact from half an hour to three to eight hours.
Extracorporeal shock wave therapy (ESWT) may be offered in order to improve penile pain. The mechanism of action involved in this procedure remains unclear, but is based on two hypotheses. First, it is thought that ESWT may directly damage and remodel the penile plaque. Second, it is hypothesized that ESWT generates heat, and therefore increases the vascularity, resulting in an inflammatory reaction involving plaque lysis by macrophage activity and resulting in plaque resorption. However, the AUA reiterates that it should not be used for the reduction of penile curvature or plaque size.
Initial conservative treatment of Peyronie disease is recommended for patients in the early stage when symptoms are present and the plaque is not densely fibrotic or calcified. No single drug has been approved by the European Medical Association for the treatment of Peyronie disease. Clinicians should discuss with patients the available treatment options with the corresponding benefits and risks associated with each.
Helpful treatments
Surgery may be unnecessary when dealing with the chronic phase. Drugs are more effective in the reduction of curvature and pain due to Peyronie’s disease. It should be noted that medications can also significantly contribute to the treatment of this condition especially when combined with traction therapies.
Surgical treatment methods
This procedure is typically not recommended except for severe conditions that are unresponsive to medications. For instance, surgery may be advisable if it leads to serious problems during sexual intercourse or causes a lot of pain within twelve to eighteen months.
Surgery may be considered for patients who are in the stable or chronic phase of the disease, which is defined as stable symptoms and curvature for at least 3 months. Some authors have suggested that surgery may be performed for individuals with severe penile curvatures without loss of erection. It is important to note that there are different surgical approaches which may be indicated based on the severity of the curvature.
Some common surgical techniques are:
- Plication: During this surgery, the expert removes a piece of the tunica albuginea from the penis’s side to help straighten it. Several methods are applicable, but they ultimately depend on the urologist’s experience. The AUA guidelines recommend penile plication procedures for an angulation smaller than 70 degrees, while incision and grafting procedures are recommended for a penile angulation larger than 60 to 70 degrees. These penile lengthening procedures involve performing an incision in the concave side of the tunica to increase the length, creating a defect that may be covered by a graft. However, this technique has been associated with high rates of postoperative erectile dysfunction.
- Penile Implants: This procedure is considered if a person has both Erectile Dysfunction and Peyronie’s disease. During the procedure, the surgeon implants a device that may help erection by straightening the penis. Penile prosthesis surgery may be offered to patients with PD with erectile dysfunction and/or penile deformity sufficient to prevent intercourse.
- Grafting: The urologists make one cut or more in the scar tissue. These cuts enable the sheaths to stretch out and straighten the penis. The surgeon may remove some scar tissue. After the procedure, men may experience ED or numbness of the penis. Additional intra-operative procedures, such as modelling, plication or incision/grafting, may be performed when significant penile deformity persists after insertion of the penile prosthesis.
Several conditions determine the type of surgery. Factors like the position of scar tissue, level of symptoms, and others may be necessary determinants that the surgeon may review. During surgery, doctors may also need to perform circumcision on those that aren’t circumcised.
Conclusion
Peyronie’s disease could prove to be troublesome since it affects men’s sex life. It also affects mental and psychosocial health since it can cause depression, anxiety, and fear. Despite all the options to treat Peyronie’s, the surgical intervention would still prove to be the most viable option with reliable results. It is also an utmost importance to consult with a doctor once the symptoms are noticed to make necessary interventions as soon as possible.
Outlook
At the moment, the exact cause of Peyronie’s remains unknown. However, several studies have been undertaken to determine its etiology.
The disease may seem to have a significant effect not only on an individual’s physical condition but also on one’s mental and psychosocial health. The degree of pain and discomfort it causes is highly unhealthy. In some men, it leads to depression, anxiety, and fear.
Although there are a variety of treatment options for this disease, surgery remains to be the most viable option with long-lasting results. It is also worth emphasizing that in rare cases (less than 10%), spontaneous resolution occurs, where the plaque hardens and the pain resolves. Holistic treatment of the afflicted individual includes medical, surgical, as well as psychosocial methods.
Overall, it is advisable to seek medical attention once symptoms are noticed, and for patients to follow set guidelines that may help improve one’s quality of life.
Free Resources
References
- Aita, Giuliano, Ros, Carlos Teodósio da, Silvinato, Antonio, & Bernardo, Wanderley Marques 2019, ‘Peyronie’s disease: clinical treatment’, Revista da Associação Médica Brasileira, vol. 65, no. 10, pp. 1231-1239. Epub November 07, 2019. https://doi.org/10.1590/1806-9282.65.10.1231
- Ali Can Albaz, Oktay Ucer 2017, ‘Peyronie’s Disease: Recent Treatment Modalities’, EMJ, vol. 2, no. 3, pp. 63-70 https://www.emjreviews.com/urology/article/peyronies-disease-recent-treatment-modalities/
- Capoccia, E. and Levine, L.A., 2018. Contemporary review of Peyronie’s disease treatment. Current urology reports, 19(7), p.51. https://pubmed.ncbi.nlm.nih.gov/29774446/
- Chen, J.Y., Hockenberry, M.S. and Lipshultz, L.I., 2018. Objective assessments of Peyronie’s disease. Sexual med. reviews, 6(3), pp.438-445. https://sci-hub.tw/10.1016/j.sxmr.2017.12.006
- Fernandes, M., de Souza, L., & Cartafina, L. P, 2018, ‘Ultrasound evaluation of the penis’, Radiologia brasileira, vol. 51, no. 4, pp. 257–261. https://doi.org/10.1590/0100-3984.2016.0152
- Hatzimouratidis, K., Eardley, I., Giuliano, F., Hatzichristou, D., Moncada, I., Salonia, A., Vardi, Y. and Wespes, E., 2012. EAU guidelines on penile curvature. European urology, 62(3), pp.543-552. https://uroweb.org/wp-content/uploads/Hatzimouratidis-K-et-al-Eur-Urol-2012-623543-EAU-Guidelines-on-penile-curvature.pdf
- Hussein, Ahmed A; Alwaal, Amjad; Lue, Tom F, 2015, ‘All about Peyronie’s disease’, Asian Journal of Urology, vol. 2, no. 2, pp. 70-78, https://www.sciencedirect.com/science/article/pii/S2214388215000430
- Jalkut M 2003, ‘Peyronie’s Disease: A Review’, Reviews in Urology, vol. 5, no. 2, pp. 142-148 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1473022/
- Kuehhas, F. E., Weibl, P., Georgi, T., Djakovic, N., & Herwig, R., 2011, ‘Peyronie’s Disease: Nonsurgical Therapy Options’, Reviews in urology, vol. 13 no.3, pp. 139–146. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3221554/
- Laurence A Levine, 2006, ‘Peyronie’s disease and erectile dysfunction: Current understanding and future direction’, Indian Study of Urology, vol. 22, no. 3, pp. 246-250. https://doi.org/10.4103/0970-1591.27633
- Mohede, D.C., de Jong, I.J. and van Driel, M.F., 2019. Medical treatments of Peyronie’s disease: past, present, and future. Urology, 125, pp.1-5. https://pubmed.ncbi.nlm.nih.gov/30634029/
- Nehra, A., Alterowitz, R., Culkin, D.J., Faraday, M.M., Hakim, L.S., Heidelbaugh, J.J., Khera, M., Kirkby, E., McVary, K.T., Miner, M.M. and Nelson, C.J., 2015. Peyronie’s disease: AUA guideline. The Journal of urology, 194(3), pp.745-753.https://www.auanet.org/guidelines/peyronies-disease-guideline
- Rosai, J. & Ackerman, L. (2011). (2011). Rosai and Ackerman’s surgical pathology. Edinburgh, Mosby.
- Segal, R. L., & Burnett, A. L., 2013, ‘Surgical Management for Peyronie’s Disease’, The world journal of men’s health, vol. 31, no. 1, pp. 1–11. https://doi.org/10.5534/wjmh.2013.31.1.1
- Tsambarlis, P. and Levine, L.A., 2019. Nonsurgical management of Peyronie’s disease. Nature Reviews Urology, 16(3), pp.172-186. https://www.nature.com/articles/s41585-018-0117-7
- Tunuguntla, H.S.G.R., 2001. Management of Peyronie’s disease–a review. World journal of urology, 19(4), pp.244-250. https://sci-hub.tw/10.1007/s003450100209