


News
Summary
There are lots of neurological causes of sexual dysfunction in men specifically, erectile dysfunction. The neurological causes of ED are broad and can be divided into primary, secondary, and tertiary causes. Some of the top primary neurological causes which includes Parkinson’s disease and epilepsy, and each of their implications will be discussed in this article.
Introduction
There are many neurological causes of sexual dysfunction in men (SDM). As a neurosurgeon I often consider sexual dysfunction in men with a neurological basis divided into primary, secondary, and tertiary causes. Symptoms of sexual dysfunction may include;
- loss of libido,
- uncomfortable or painful intercourse,
- premature ejaculation,
- difficulty maintaining and/or achieving an erection,
- and decreased frequency of ejaculation.
In this article, we shall explore several neurological disorders in which sexual dysfunction in men is prominent, and I will share with you my own experience in attempting to help men with this frustrating problem.
Before addressing sexual dysfunction of a neurological origin it is essential to consider the patient’s attitude towards sex, sexual orientation, and cultural influences. Neurological sexual dysfunction can have a devastating effect on a man’s overall quality of life as well as significant effects on his sexual partner.
Broad neurological causes of ED
- Primary sexual dysfunction is often due to lesions affecting the neural pathways for normal sexual function
- http://telegraphharp.com/wp-json/oembed/1.0/embed?url=http://telegraphharp.com/ Secondary sexual dysfunction is due to;
- disability caused by poor bladder and bowel control, fatigue, muscle weakness, spasticity, immobility, tremor, cognitive impairment, and sensory problems,
- non-neurological co-morbidities, e.g., hypertension, diabetes, depression, hypercholesterolemia, obesity, and chronic smoking, or
- medications used to treat the neurological conditions (spasticity, urinary frequency, sensory pain, etc.) or non-neurological co-morbidities (hypertension, diabetes, depression, etc.)
- peerlessly Tertiary sexual dysfunction relates to the psychological, social, and cultural issues that affect sexual response. These variables can include;
- anxiety,
- low self-esteem,
- altered marital and family roles,
- changes in body image,
- and fear of rejection by the partner
Primary neurological causes of sexual dysfunction
In this article, we shall discuss the following primary neurological causes of men’s sexual dysfunction:
- Multiple Sclerosis (MS)
- Parkinson’s Disease (PD)
- Spinal Cord Injury (SCI)
- Epilepsy
- Peripheral Neuropathy (PN)
Primary neurological sexual dysfunction is due to lesions or altered functions in some portion of the nervous system involved in the normal male sexual process. Various areas of the brain, brainstem, pathways in the spinal cord, spinal nerve roots, peripheral nerves, and the autonomic nervous system all contribute to normal male sexual function.
Primary neurological sexual dysfunction in men can result from any of the following conditions:
1. Multiple Sclerosis (MS)
Although more common in women, MS also affects men. As the name suggests, MS is “multiple,” which refers to its propensity to occur at many different locations in the nervous system and at many other times. MS tends to have a “waxing and waning” course with onset of symptoms, leveling off, and then decreasing or disappearing. To be followed at a later time with symptoms related to another location in the nervous system. Sometimes MS is steadily progressive and fatal.
Sexual dysfunction in men with MS also tends to have a variable course. Demyelination or loss of the myelin sheath can occur in any part of the brain, brainstem, or spinal cord with associated SDM along with other neurological symptoms such as visual loss, double vision, paralysis, loss of sensation, or loss of balance. The degree of sexual dysfunction experienced by men with MS can vary significantly from a slight difficulty in achieving or maintaining an erection to complete loss of libido and inability to achieve an erection.
As a neurosurgeon, I did not usually manage MS, a condition traditionally managed by neurologists. On occasion, however, I was involved in the initial evaluation of men with sexual dysfunction and other neurological symptoms of unknown origin that proved eventually to be due to MS. One such case is often on my mind since it represents an error in diagnosis that I did not discover at first.
A 32-year-old man was referred to me because of a loss of vision. His only other symptom was difficulty in obtaining and maintaining an erection of only about six weeks duration. On examination, he had left homonymous hemianopsia or loss of vision in the left half of both visual fields. An MRI scan revealed a slightly enhancing lesion about 3.5 cm in diameter just adjacent to the posterior horn of the right lateral ventricle of his right hemisphere. I carried out a stereotactic biopsy of the lesion that was described by the pathologist in the frozen section to be a low-grade glioma. Since the stereotactic frame was already in place and after discussion with the patient, we decided to proceed immediately to treat the lesion with stereotactic radiosurgery with the Gamma Knife. Forty-eight hours later, the pathologist informed me that the lesion was due to MS and was not a glioma! Had I known that, I would, of course, not treated the patient with radiosurgery. Fortunately, over time the MS lesion resolved, and the patient experienced no complications of the unnecessary treatment. His visual defect was also resolved. During a further follow-up of over ten years, the man experienced no additional episodes of MS.
Oral treatments are the main treatments used to treat male sexual dysfunction related to MS. Three different studies confirmed an excellent response to these treatments, with up to 89% of men achieving a normal erection. On the other hand, one study failed to show improvement when the treatment was compared to a placebo. This could potentially indicate a psychological aspect interfering with normal sexual function or quite a severe erectile dysfunction.
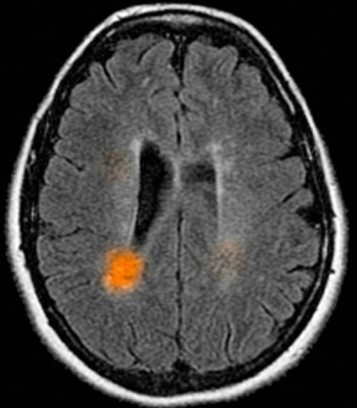
Multiple Sclerosis lesion causing visual field defects and male sexual dysfunction 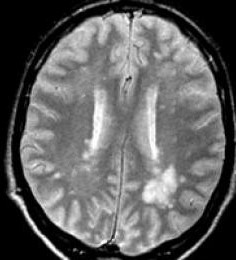
Multiple Sclerosis lesion causing visual field defects and male sexual dysfunction
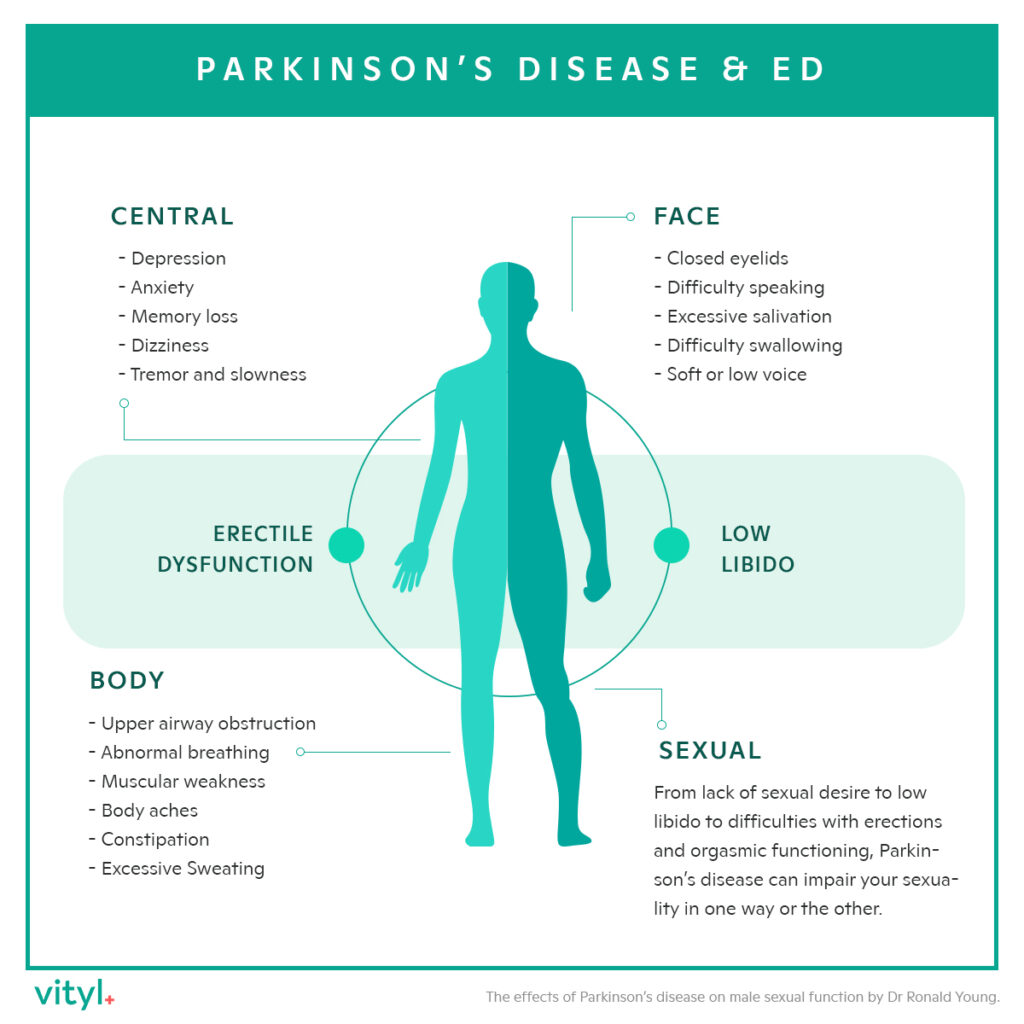
2. Parkinson’s Disease (PD)
Neurosurgeons are increasingly included in the treatment of Parkinson’s disease. Parkinson’s disease is a neurodegenerative disease that is steadily progressive, although the time course of progression is quite variable. Some patients experience a steady progression to death within 1-2 years after the onset of symptoms. In contrast, others have a long passage of symptoms over many, many years with death due to intercurrent problems like pneumonia. In my long career as a neurosurgeon, I have been involved in the treatment of hundreds of patients with Parkinson’s disease. In the days before the treatment of Parkinson’s disease, we neurosurgeons used ablative procedures like thalamotomy and pallidotomy to treat Parkinson’s disease. In recent years neuromodulation techniques, particularly Deep Brain Stimulation (DBS) has become the treatment of choice for Parkinson’s disease.
Parkinson’s disease is a primary motor disorder that involves the brain and brainstem. Interestingly, men but not women with Parkinson’s disease often experience sexual dysfunction. The common symptoms of sexual dysfunction in men with Parkinson’s disease are decreased desire, erectile dysfunction, difficulties in reaching orgasm, and sexual dissatisfaction. Unfortunately, some men with Parkinson’s disease suffer from hypersexuality primarily related to treatment with dopamine.
Some fifteen years ago, I was referred a 58-year-old man with slowly progressive Parkinson’s disease of some eight years duration. His primary symptoms were rest tremors in both upper extremities and some rigidity, but his main complaint was ED despite normal sexual urges and a willing partner. We discussed the use of deep brain stimulation (DBS) to treat his tremor and rigidity. I told him that it was unlikely that DBS would help his ED. Subsequently, I place bilateral thalamic DBS leads during staged operations one month apart. He had immediate and nearly complete resolution of his tremor, marked improvement in his rigidity, and to my amazement, his ED disappeared as well. In a follow-up lasting over fifteen years, he showed slow progression but was alive and functional at age 73 when I last saw him.
Not all men with sexual dysfunction related to Parkinson’s disease are candidates for deep brain stimulation. In a study of 116 men with sexual dysfunction due to Parkinson’s disease, oral medication produced a normal erectile dysfunction score in nearly 57% of treated men compared to only about 9% in the placebo-treated group.
3. Spinal Cord Injury (SCI)
The acute management of spinal cord injury (SCI) is often performed by neurosurgeons. Long-term management of the side effects of spinal cord injury, such as sexual dysfunction, is usually managed either by neurologists or by physicians who specialize in the care and treatment of spinal cord injury patients. During my first year as a neurosurgical resident at the Veterans Administration Hospital in Long Beach, CA, I had the opportunity to observe many patients with severe spinal cord injury. They were treated in a unique spinal cord injury Unit at that hospital. I saw many men who had a partial or complete loss of sexual function for whom, at that time, there was no effective treatment. Fortunately, for these men, the clinical efficacy of oral treatment is well documented. Furthermore, the effectiveness of these medications over follow-up periods as long as ten years is also proven.
4. Epilepsy
As many as 50% of men with epilepsy suffer from sexual dysfunction, mainly arousal disorders such as erectile dysfunction and premature ejaculation. Men with epilepsy face a two to four-fold increase in sexual dysfunction compared to the general, healthy, male population. Multiple mechanisms, including direct effects of epilepsy, effects of treatment, and psychosocial factors, contribute to sexual dysfunction in epilepsy. Some evidence suggests that seizures and interictal epileptiform discharges can directly affect the hypothalamic-pituitary axis as well as the production of hormones. LowT levels may be contributors to sexual dysfunction in men with epilepsy, but “concentrating on hormone levels alone as an explanation of sexual dysfunction in epilepsy represents an overly simplistic approach to the problem,” according to one study. Comorbid neuropsychological conditions such as anxiety and depression can also contribute to sexual dysfunction in men with epilepsy.
Neurosurgeons have become increasingly involved in the treatment of epilepsy, particularly temporal lobe epilepsy and other forms of focal as opposed to generalized epilepsy. Surgical studies often lament the fact that many patients with surgically-treatable epilepsy are not referred for surgery even though their seizures have failed to respond to multiple antiepileptic drugs for many years. Improvements in quality of life and cognitive function often occur after surgical resection of focal temporal lobe epilepsy, but effects on sexual dysfunction are usually not evaluated. One study provided evidence that early and effective epilepsy surgery may not only render the patient with intractable partial epilepsy seizure-free but also allows the individual to become a participating and productive member of society.
On the other hand, some studies have specifically addressed the question of sexual function in patients who have undergone surgical treatment of epilepsy. As many as 64% of patients who underwent surgical resection of a temporal lobe epileptic focus reported improvements in their sexual functions. In a study of fifty married men who underwent temporal lobe resection for treatment of epilepsy-related to mesial temporal sclerosis, a majority reported improvement in sexual function. However, the degree of improvement did not bring them to the same level as a group of matched normal control males. Patients who reported a postoperative increase in sexual function had a significantly larger volume of amygdala contralateral to the side of their surgery than patients with a sexual decrease or no change compared to control subjects. As one might expect, patients who are seizure-free after surgery are more likely to report a higher level of life satisfaction and sexuality than the non-seizure free group.
During my tenure as the Chairman of Neurosurgery at the University of California, Irvine, I was referred a 37-year-old married man with a ten-year history of temporal lobe epilepsy related to mesial temporal sclerosis. He was taking three different treatments but with persistent seizures that interfered with his ability to be employed. He also complained of a significant loss of sexual function, primarily ED, but also decreased libido. His wife noted how he almost always avoided any sexual contact. After a suitable workup to identify the location of his epileptogenic focus, I performed an en-bloc resection of his right temporal lobe. He had one abortive seizure three weeks after surgery. Still, in a follow-up that lasted over ten years, he had no further seizures, and he was able to wean off treatment. His sexual function returned to normal, and less than one year post-operatively, his wife bore their first child!
The withdrawal of treatment in my patient is in line with studies that confirm that it is safe to withdraw them after successful surgery and that recurrent seizures are infrequent and easily managed. Since treatments are often the sole or major contributor to sexual dysfunction, the need to withdraw them, if possible, is essential to restoring normal sexual function. However, do not stop any treatment without the assistance of your medical team.
5. Peripheral Neuropathy (PN)
Peripheral neuropathy refers to the conditions and symptoms that result when nerves that carry messages to and from the brain are no longer working correctly due to damage or disease.
Symptoms of peripheral neuropathy commonly include numbness and tingling of the feet and difficulty with balance. People with peripheral neuropathy also complain of pain in their feet and lower legs. Examination shows loss of tactile and joint position sense in the feel as well as absent lower extremity reflexes. Peripheral neuropathies have many causes, including alcoholism, smoking tobacco, diabetes, and as a remote effect of cancer, although in many cases, a specific cause is not identified. Peripheral neuropathies have been described as an undiagnosed cause of erectile dysfunction and underestimated in the pathogenesis of ED. In a group of ninety men with ED, as many as 61% showed evidence of peripheral neuropathy on electrophysiological tests, and 14% showed evidence of Pudendal Nerve neuropathy. Another study found evidence of dysfunction of large and small diameter nerve fibers in patients with ED of all etiologies.
Neurosurgeons are not usually involved in the treatment of peripheral neuropathy. Years ago, I saw a 54-year-old man with severe neuropathic pain involving both his feet and lower legs. He had undergone multiple unsuccessful treatments and was currently taking large doses as well as antiepileptic and anti-depressive treatments. He experienced severe erectile dysfunction, and his problem occurred before drugs to treat ED were available. I placed a spinal cord electrical stimulator in the epidural space at the L1-2 spinal level and advanced the paddle-shaped pad up to the T-10 level. The unit was activated by a battery-operated device placed subcutaneously. Activation of the stimulator produced paresthesias bilaterally in his legs and feet with almost complete resolution of his pain. He was eventually tapered off of all treatments with a gradual resumption of regular sexual activity.
Conclusion
Sexual dysfunction is a common symptom of a variety of neurological disorders, although it is often overlooked. Useful sexual function is an integral part of a normal psychosocial life. An inquiry into the sexual function of patients with neurological diseases is essential because many of the causes of sexual dysfunction are treatable. In most cases, the treatment of sexual dysfunction in men with neurological illnesses is non-surgical, but in certain circumstances, a neurosurgical intervention can prove life-changing.
References
- Baird, A.D., Wilson, S.J., Bladin, P.F., Saling, M.M. and Reutens, D.C., 2004. The amygdala and sexual drive: insights from temporal lobe epilepsy surgery. Annals of Neurology: Official Journal of the American Neurological Association and the Child Neurology Society, 55(1), pp.87-96. https://pubmed.ncbi.nlm.nih.gov/14705116/
- Bleustein, C.B., Arezzo, J.C., Eckholdt, H. and Melman, A., 2002. The neuropathy of erectile dysfunction. International journal of impotence research, 14(6), pp.433-439. https://pubmed.ncbi.nlm.nih.gov/12494274/
- Bronner, G., Aharon-Peretz, J. and Hassin-Baer, S., 2015. Sexuality in patients with Parkinson’s disease, Alzheimer’s disease, and other dementias. In Handbook of clinical neurology (Vol. 130, pp. 297-323). Elsevier. https://pubmed.ncbi.nlm.nih.gov/26003251/
- Bronner, G. and Hassin-Baer, S., 2012. Exploring hypersexual behavior in men with Parkinson’s disease: is it compulsive sexual behavior?. Journal of Parkinson’s disease, 2(3), pp.225-234. https://pubmed.ncbi.nlm.nih.gov/23938230/
- Cascino, G.D., 2004. Surgical treatment for epilepsy. Epilepsy research, 60(2-3), pp.179-186. https://pubmed.ncbi.nlm.nih.gov/15380562/
- Christianson, S.Å., Silfvenius, H., Säisä, J. and Nilsson, M., 1995. Life satisfaction and sexuality in patients operated for epilepsy. Acta neurologica scandinavica, 92(1), pp.1-6. https://pubmed.ncbi.nlm.nih.gov/7572053/
- Engel, J., McDermott, M.P., Wiebe, S., Langfitt, J.T., Stern, J.M., Dewar, S., Sperling, M.R., Gardiner, I., Erba, G., Fried, I. and Jacobs, M., 2012. Early surgical therapy for drug-resistant temporal lobe epilepsy: a randomized trial. Jama, 307(9), pp.922-930. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4821633/
- Fowler, C.J., Miller, J.R., Sharief, M.K., Hussain, I.F., Stecher, V.J. and Sweeney, M., 2005. A double blind, randomised study of ED treatment* for erectile dysfunction in men with multiple sclerosis. Journal of Neurology, Neurosurgery & Psychiatry, 76(5), pp.700-705. https://pubmed.ncbi.nlm.nih.gov/15834030/
- Lombardi, G., Macchiarella, A., Cecconi, F. and Del Popolo, G., 2009. Ten‐year follow‐up of ED treatment* use in spinal cord‐injured patients with erectile dysfunction. The journal of sexual med., 6(12), pp.3449-3457. https://pubmed.ncbi.nlm.nih.gov/19686427/
- Lombardi, G., Macchiarella, A. and Del Popolo, G., 2010. Efficacy and safety of ED treatment* for erectile dysfunction in patients with multiple sclerosis. The journal of sexual med., 7(6), pp.2192-2200. https://pubmed.ncbi.nlm.nih.gov/20384939/
- Lombardi, G., Musco, S., Kessler, T.M., Marzi, V.L., Lanciotti, M. and Del Popolo, G., 2015. Management of sexual dysfunction due to central nervous system disorders: a systematic review. Bju International, 115, pp.47-56. https://pubmed.ncbi.nlm.nih.gov/25599613/
- Ramesha, K.N., Radhakrishnan, A., Jiayaspathi, A., Padickaparambal, S., Alexander, A., Unnikrishnan, J.P., Sarma, P.S. and Radhakrishnan, K., 2012. Sexual desire and satisfaction after respective surgery in patients with mesial temporal lobe epilepsy with hippocampal sclerosis. Epilepsy & Behavior, 25(3), pp.374-380. https://pubmed.ncbi.nlm.nih.gov/23103313/
- Rathore, C., Henning, O.J., Luef, G. and Radhakrishnan, K., 2019. Sexual dysfunction in people with epilepsy. Epilepsy & Behavior, 100, p.106495. https://pubmed.ncbi.nlm.nih.gov/31577987/
- Rathore, C., Panda, S., Sarma, P.S. and Radhakrishnan, K., 2011. How safe is it to withdraw antiepileptic treatment* following successful surgery for mesial temporal lobe epilepsy?. Epilepsia, 52(3), pp.627-635. https://pubmed.ncbi.nlm.nih.gov/21219315/
- Rathore, C., Henning, O.J., Luef, G. and Radhakrishnan, K., 2019. Sexual dysfunction in people with epilepsy. Epilepsy & Behavior, 100, p.106495. https://pubmed.ncbi.nlm.nih.gov/31577987/
- Safarinejad, M.R., 2009. Evaluation of the safety and efficacy of ED treatment for erectile dysfunction in men with multiple sclerosis: a double-blind, placebo controlled, randomized study. The Journal of urology, 181(1), pp.252-258. https://pubmed.ncbi.nlm.nih.gov/19013598/
- Safarinejad, M.R., Taghva, A., Shekarchi, B. and Safarinejad, S., 2010. Safety and efficacy of ED treatment in the treatment of Parkinson-emergent erectile dysfunction: a double-blind, placebo-controlled, randomized study. International journal of impotence research, 22(5), pp.325-335. https://pubmed.ncbi.nlm.nih.gov/20861846/
- Talbot, J.A., Sheldrick, R., Caswell, H. and Duncan, S., 2008. Sexual function in men with epilepsy: how important is T level?. Neurology, 70(16), pp.1346-1352. https://pubmed.ncbi.nlm.nih.gov/18413588
- Valles‐Antuña, C., Fernandez‐Gomez, J. and Fernandez‐Gonzalez, F., 2011. Peripheral neuropathy: an underdiagnosed cause of erectile dysfunction. BJU international, 108(11), pp.1855-1859. https://pubmed.ncbi.nlm.nih.gov/21592291/
- Zhao, S., Tang, Z., Xie, Q., Wang, J., Luo, L., Liu, Y., Zhu, Z., Luo, J. and Zhao, Z., 2019. Association between epilepsy and risk of sexual dysfunction: A meta-analysis. Seizure, 65, pp.80-88. https://www.seizure-journal.com/article/S1059-1311(18)30447-3/fulltext
- Zhao, S., Wang, J., Xie, Q., Luo, L., Zhu, Z., Liu, Y., Luo, J. and Zhao, Z., 2019. Parkinson’s Disease Is Associated with Risk of Sexual Dysfunction in Men but Not in Women: A Systematic Review and Meta-Analysis. The Journal of Sexual Med., 16(3), pp.434-446. https://pubmed.ncbi.nlm.nih.gov/30773498/






